Manual Muscle Testing A Thing of the Past?
Hand-Held Dynamometers may quickly replace subjective manual techniques
Dr. James Fung, BSc, DC, RTP
Canadian Chiropractor-Vol 8, No 4, June/July 2003
Dr. James Fung graduated from the University of Toronto in 1997 with a Hon BSc degree in molecular genetics. He is a 2001 graduate of CMCC. He currently maintains two practices in Toronto. He is also a certified instructor in the Trigenics seminar series.
Manual muscle testing (MMT) is commonly used by clinicians and therapists as a tool for assessment and diagnosis. There are two major roles of MMT in a chiropractic clinical practice as an indicator to augment or confirm a normal exam such as that used in applied kinesiology (1) and to measure the strength of a muscle and identify areas of muscular weakness due to injury or disease.
By locating weakness, not by confirming strength, MMT provides clinicians with a useful diagnostic tool. The problem with traditional MMT is that the results are subject to nature. (2)
Noreau showed the sensitivity of the MMT method is insufficient to assess muscle strength, at least for grade 4 and higher, and to detect small or moderate increases of strength over the course of rehabilitation. (3) In addition, Frese et al. also showed that the accuracy and reliability of MMT is questionable. (4)
Various types of hand-held dynamometers (HHD) were developed in an attempt to eliminate the inherent problems with MMT. In this article we will discuss the use of various models of HHD to obtain objective, measurable muscle strength results.
Models of HHD
Hand-held dynamometers provide a simple, quick, portable, and non-invasive means of measuring isometric muscle strength. Clinicians and researchers commonly use either:
Modified sphygmomanometers (modified pressure cuffs)
Spring gauge dynamometers
Strain gauge dynamometers (5)
The modified sphygmomanometer is easy and inexpensive to use, but values above 210 mm Hg have a curvilinear relationship with other strength-testing devices. Higher pressures against the bladder cuff may exceed the underlying pressure within the cuff to the point that the sphygmomanometer values drop off at the higher end of the scale. Therefore, it may not be the best choice for obtaining accurate strength measurements of stronger muscles. (6) Unlike modified sphygmomanometers, spring gauge dynamometers have a linear relationship with certified weights throughout the 27 kg range. However, they tend to lose accuracy with extended use. (5) Strain gauge dynamometers are the most sensitive. They maintain a linear relationship with certified weight values. The sensitivity and accuracy of a strain gauge dynamometer helps to rule out the instrument as a source of poor reliability. (5) Commercially available strain gauge dynamometers include MicroFET, Ametek Accuforce III, MEED 3000 and the Nicholas Manual Muscle Tester.
The MicroFET is a battery-operated, electromechanical device. It measures, freezes, and displays the peak force and time duration of muscle testing. The MicroFET 3 model is sensitive to 0.1 lb. Studies also show that strain gauge dynamometers exhibit good reliability and good validity for measuring muscle strength. (5,7)
There are several aspects of muscle testing procedures that must be considered:
The tester strength must be high relative to the forces being measured.
Reproducibility of results depends on the clinician¹s experience.
The time of day as some patients may fatigue as the day progresses.
Proper stabilization and position of the patient and the tester.
The dynamometer must be perpendicular to the limb segment during the tests.
Angle of the joint during testing.
Repeat trial consistency (2-3x).
Some of the HHD devices available on the market such as the MicroFET models (Diagram 2) may be connected to a computer software system, which will record and analyze the results.
Dynametric Muscle Testing (DMT) validity is based on:
Repeat consistency
Ten per cent between repeated trials
The presence of cogwheel release
Regional weakness that has no neuroanatomic basis
The interpretation of the time-force curves
The presence of overreaction behaviour.
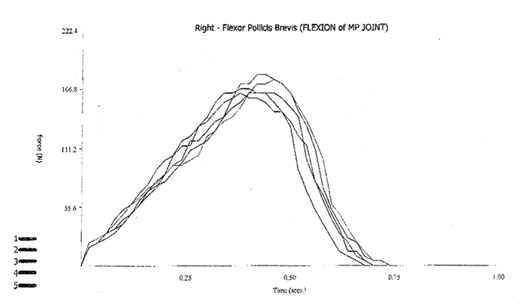
Figure 1
An example of the muscle testing results profile of a rightflexor pollicis brevis. The graph shows the force distribution overtime of five consecutive trial tests.
The program allows the evaluator to ensure the repeated trials are consistent. In addition, the MicroFET 3 model also functions as an inclinometer in the same unit (Diagrams 3 & 4).
The unit calculates the range of motion by recording the difference between the starting position and the end position of a specific range of motion.

Diagram 3 Starting Position Diagram 4 Finishing Position
Reference Values
Since muscle force and functional ability are not related linearly, maximum force can be reduced while functional ability is still maintained. (8) For diagnostic and therapeutic reasons, loss of muscle force should be detected as early and accurately as possible. (8) Over the recent years studies have provided reference values for different age groups for muscle strength obtained by HHD. (8,9,10) Most of these reference values are established for extremity movements. These age-related reference values can be employed in a clinical setting to document whether an individual is impaired relative to a healthy population of the same gender and age. These values can also help to estimate the severity of force-generating impairments in patients, to quantify muscle weakness in individual muscle groups and to evaluate the effects of therapy. (8,9,10)
In summary, without an HHD, the clinician normally assigns a value to the test results, such as 1 to 5 or good-fair-poor, depending on how much force the clinician thought the patient exerted. Problems arise, however, trying to assign a score based on subjective feeling, especially when the patient is re-tested at a later date. Many of the problems inherent to manual muscle testing can be resolved by using an HHD.
References:
MicroFET3 The User Guide.
Noreau L, Vachon J. Comparison of three methods to assess muscular strength in individuals with spinal cord injury. Spinal Cord 1998 Oct; 36(10): 716-23.
Frese E. et al. Clinical reliability of manual muscle testing; Middle trapezius and gluteus medius muscles. Phys Ther 1987 Jul; 67(7): 1072-6.
A. Williams Andrews PT, Hand-held dynamometry for measuring muscle strength, Journal of Human Muscle Performance 1991; 1 (1) 35-50.
Bohannon RW, Lusardi MM. Modified sphygmomanometer versus strain gauge hand-held dynamometer. Arch Phys Med Rehabil 1991; 72 (11): 911-4
Bohannon RW. Intertester reliability of hand-held dynamometry: a concise summary of published research. Percept Mot Skills 1999 Jun; 88: 899-902.
Beenakker EA Et al. Reference values for isometric muscle force obtained in 270 children aged 4-16 years by hand-held dynamometry. Neuromuscul Disorder 2001 Jul; 11(5): 441-6.
Bohannon RW. Reference values for extremity muscle strength obtained by hand-held dynamometry from adults aged 20-79 years. Arch Phys Med Rehabil 1997 Jan; 78 (1): 1442-3.
Andrews AW, Et al. Normative values for isometric muscle force measurements obtained with hand-held dynamometers. Phys Ther 1996 Mar; 76(3): 248-59.