Hybrid Therapy Aims to Re-establish Neuromuscular Balance
RBy Dr. Richard M. Cleland
Frozen shoulder syndrome (FSS), or adhesive capsulitis, is commonly used as the clinical diagnosis of choice for most painful shoulder conditions that are associated with a global loss of motion of the glenohumeral joint. However, given the degree of movement that is lost, it is interesting to note that FSS is rarely the result of any serious underlying pathology. Grubbs’ definition of frozen shoulder syndrome is “a soft tissue capsular lesion accompanied by painful and restricted active and passive motion at the glenohumeral joint.”(1,2)
The onset of FSS is usually preceded by a physically traumatic event, followed by a period of time where the shoulder joint becomes progressively more restricted and painful. However, in a significant number of cases, no specific physical trauma can be attributed to the shoulder’s dysfunction. Recent statistics suggest that FSS affects from 2 to 5% of the population, with a female:male ratio of 60:40.(1,2,4-7) Up to 15% of patients will experience FSS bilaterally. The most prevalent age group appears to be between 40 and 60 years, and FSS is five times more common in diabetics.(3) Given the somewhat idiopathic nature of FSS, several theories have been proposed to explain its origin.(1,3,8) Hormonal, genetic and autoimmune theories have been suggested, but are difficult to prove to date. The most likely theory to explain the underlying cause is postural deviation – the most convincing study has indicated that “long-standing round-shouldered posture causes a shortening of the shoulder ligaments, which then makes the patient predisposed to FSS.”(4-6)
Given the above information, any therapy which could address the neuromuscular component of the glenohumeral joint may be deemed appropriate. Trigenics®, a revolutionary new neuromuscular therapy, has emerged as a perfect option to provide treatment for this syndrome. Trigenics® is a hybrid therapy, combining the benefits of three already well-established treatment protocols: soft-tissue manipulation, biofeedback and acupuncture meridian therapy. The goal of Trigenics® is to restore the proper “tone” of any given muscle, thereby re-establishing a correct neuromuscular balance, and better strength-tension relationships for optimum muscular contraction. The result is not only a muscle that responds appropriately to its neurological signal, but also restored joint biomechanics, as the joint must rely upon the surrounding muscles for movement. Finally, with an additional effect on the mind-body connection (by using influential acupuncture meridian points during its application), the amazing results that are achieved by using Trigenics® may be due to its more “holistic” approach to health and healing. Patients are often obtaining dramatic reductions in pain and incredible improvements in their conditions where other forms of therapy have failed.
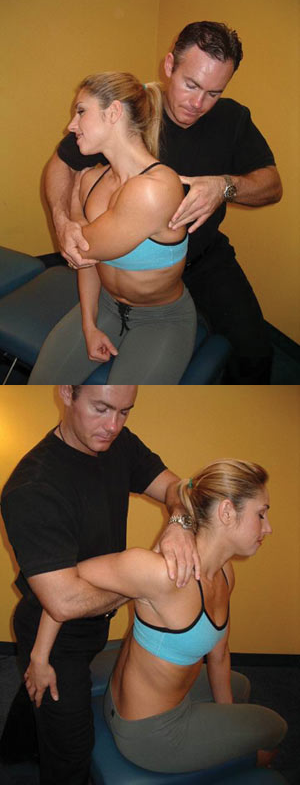 Using a model, Dr. Cleland demonstrates a Trigenics® Lengthening procedure for anterior deltoid (left) and teres minor (right).
Using a model, Dr. Cleland demonstrates a Trigenics® Lengthening procedure for anterior deltoid (left) and teres minor (right).
Case Study: Frozen Shoulder Syndrome
A 52-year-old diabetic male injured his left shoulder after lifting an object that weighed approximately five pounds. After receiving and examining the patient’s X-rays, which were used to rule out any obvious pathologies, the patient’s medical doctor diagnosed him with frozen shoulder syndrome. The patient was prescribed pain medication and physiotherapy. After six to seven months of physiotherapy, the patient expressed dissatisfaction with the lack of improvement and began to seek out new treatment options. Upon learning about Trigenics, the patient presented to our clinic for a trial of Trigenics® combined with chiropractic care.
In the initial examination, observation revealed that the patient’s left shoulder was elevated at least three inches higher than his right. Palpation of the patient’s left shoulder revealed hypertonicity in the upper trapezius, levator scapulae, supraspinatus, infraspinatus, scalenes, sternocleidomastoid, posterior cervicals, and the pectoralis major and minor muscles. The patient was also so uncomfortable that he was unable to lie prone on the chiropractic table, with an inability to allow his left shoulder to rest level with his right shoulder.
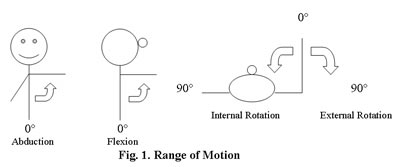
While standing, the patient’s arm abduction, flexion and external rotation were all reduced by at least 50%, with extreme pain and an observable deficit in the quality of muscular contraction in the shoulder muscles. The range of motion of the shoulder joint was measured using a hand-held goniometer (Graham-Field, Inc.).(9) Eccentric-load muscle testing was used to evaluate the integrity and strength of the shoulder’s surrounding muscles.(10) The initial testing revealed weakness in the deltoids, rhomboids, trapezius, pectoralis minor, hip flexors and gluteals bilaterally. Left-side weakness was noted in the scalenes, sternocleidomastoid, supraspinatus, infraspinatus, levator scapulae, subscapularis and pectoralis major.
The patient’s spine was assessed for vertebral subluxations using spinal kinesiopathology, neuropathophysiology, myopathology, histopathology and pathophysiology as diagnostic criteria. During the initial examination, vertebral subluxations were found at the sacroiliac (SI) joints bilaterally, cervical (C) vertebrae C1-C3, C5, C7, and thoracic (T) vertebrae T1, T5-T6, T11-T12.
Treatment was focused on addressing two main factors: systematically removing the vertebral subluxations in the patient’s spine using chiropractic adjustments, and restoring the proper integrity of the involved musculature using Trigenics. The overall objectives of treatment were to restore neuromuscular balance and thus increase the mobility of the shoulder.
During each treatment, the chiropractor would only adjust the vertebral subluxations that were indicated upon motion palpation and orthopedic assessment.
There were two possible types of applications for each muscle treated using Trigenics. The first is known as the Trigenics® Strengthening (TS) procedure, and this is indicated where a muscle tests “weak” following eccentric-load muscle-testing, or where meridian pathways require a “tonifying” effect in the flow of vital energy along that meridian channel. The second is called the Trigenics® Lengthening (TL) procedure, and in this case was used when a muscle tested “strong” following eccentric-load muscle testing, yet the associated joint still demonstrated a reduced range of motion due to muscle shortness, or when a meridian pathway required a “sedating” effect in the flow of vital energy along that meridian channel.(11,12)
The patient underwent 10 trial treatments over a course of eight weeks using a combination of Trigenics® neuromuscular therapy and chiropractic adjustments to the spine. The dramatic results of treatment are presented in Tables 1 through 3.

Conclusion
The results of this study suggest that Trigenics® is a very effective treatment tool used in combination with chiropractic adjustments to treat a condition known as frozen shoulder syndrome. FSS is often a very challenging and difficult condition, and typically requires a lengthy trial of physical therapy. The results in this case study are typical when using Trigenics® technique in conjunction with chiropractic treatment. Similar results have been demonstrated in treating a broad spectrum of conditions such as fibromyalgia, cerebral palsy, rhomboid decelerator dysfunction syndrome, Achilles paratenonitis, acute inversion ankle reflexogenic strain, and tendon-itis.(13-19)
Chiropractors wishing to treat these and other neuromuscular conditions should therefore consider adding Trigenics® to their therapeutic toolbox. •
References:
1. Niel-Asher S. Frozen shoulder syndrome. Osteopath. Dec 2000/Jan 2001; 21-23.
2. Grubbs N. Frozen shoulder syndrome – a review of literature. JOSPT Sept 1993; 18(3).
3. Pal B. et al. Limitation of joint mobility and shoulder capsulitis in insulin and non-insulin dependent diabetes mellitus. Br J of Rheumatology 1986; 25: 147-151.
4. Parker JN. Parker, PM. (editors) The Official Patient’s Sourcebook on Frozen Shoulder: A Revised and Updated Directory for the Internet Age. Chapter 1.
5. Cluett J. Basic information about adhesive capsulitis. Medical Multimedia Group, Inc. June 2, 2003.www.orthopedics.about.com/cs/frozenshoulder/a/frozenshoulder.htm
6. www.frozenshoulder.com
7. Stucky A. Keeping your cool about a frozen shoulder. Part I & II. About Physiotherapy.www.physicaltherapy.about.com/cs/shoulderinjuries/a/frozen_shoulder.htm
8. Reeves B. The natural history of the frozen shoulder. Scandinavian Journal of Rheumatology 1975; 4: 193-196.
9. Magee DJ . Orthopedic physical assessment. 3rd edition. Toronto: WB Saunders Co., 1997: Chapter 5.
10. Kendall FP. Muscles, Testing and Function 4th edition. Philadelphia: Lippincott Williams & Wilkins, 1993.
11. Austin AO. Trigenics, Theory Module I, The Trigenics® Institute of Neuromuscular Medicine.
12. Allan N. Trigenics® Neurophysiology, a description and preliminary thoughts towards a rationale, Trigenics® Clinical Applications Module III, 1st edition; 48-49.
13. DeFinney J. Achilles paratenonitis: A therapeutic case study. Canadian Chiropractor Oct 2001.
14. Pisarek S. Trigenics: A new paradigm in soft tissue therapeutics – rhomboid decelerator dysfunction syndrome. Canadian Chiropractor Feb 2001; 6(1):18, 41.
15. Pisarek S. Acute inversion ankle reflexogenic strain. Canadian Chiropractor September 2002; 7(4).
16. Guenette C. Soft tissue approach to fibromyalgia: A new treatment protocol combining chiropractic with the Trigenics® technique. Canadian Chiropractor Feb 2003; 8(1).
17. Guenette C. Rotator cuff tendonitis – case study: An application of the Trigenics® technique. Canadian Chiropractor Feb 2002.
18. Hooper K. Advanced neuromuscular medicine for soft-tissue conditions and athletic enhancement: Gluteus medius strain in a competitive triathlete – A case study. Dynamic Chiropractic Aug 16, 2003; 21(17).
19. McAllister P. Cerebral palsy – Case study. Canadian Chiropractor May 2003; 8(3); 18-23.